People with prediabetes (mostly diagnosed by IGT or IFG) should be checked annualy for T2DM. Ok, this doen't prevent anything, it's just early diagnosis.
LIFESTYLE INTERVENTIONS
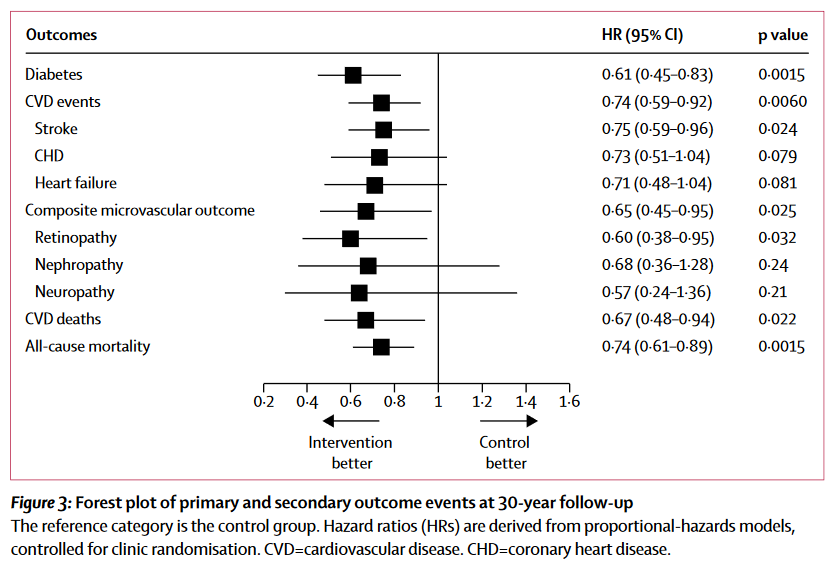
- Refer people with prediabetes to an intensive program analogous to DPP (Diabetes prevention program) that includes achievement and maintainment of 7% weight lose and at least 150 min/week of light physcal activity like bisk walking. DPP reduced diabetes incidence by 58% in 3 years. Da-Quing, a similar trial, obtained in 30 years reduction in global death (Hazard ratio 0.74), CV death (HR 0.67), CV events (HR 0.74) and microvascular complications (HR 0.65) (see figure).
- These programs have proved to be cost-effective.
- A variety of diets are acceptable for this purpose.
- Technology-assisted interventions, like smartphone-apps, may be useful.
PHARMACOLOGICAL INTERVENTIONS
- Consider metformin in prediabetes for younger (<60), obese (BMI >=35) and women with previous GDM. In DPP metformin was initially less effective than diet and exercise, but in the aforementined groups was particularly useful.
- Measure vitamin B12 in those taking metformin. There can be deficiency.
PREVENTION OF CV DISEASE
- Screen for hypertension and dyslipidemia in prediabetes due to its high CV risk.
DIABETES SELF-MANAGEMENT EDUCATION AND SUPPORT
- DSME is effective in preventing prgression from prediabetes to diabetes. The problem is it's generally not included in health programs, but the ADA recommends DSME in prediabetes, not only in diabetes.


